
What Is Creatine? A Women’s Health Guide from Menstruation to Menopause
Creatine is one of the most researched sports supplements in the world, but the story has often focused on young male athletes. That is finally changing. New research is asking a fresh question: what is creatine doing in women’s bodies, from the first period through pregnancy and right into menopause?
This article unpacks what creatine is, who has traditionally used it, and why women are now a key focus in 2025 research on hormones, brain health and ageing. We will walk through potential benefits, realistic risks, and why product quality (including German-made Creapure) matters. This is general education only – you should discuss any supplement decisions with your GP or Accredited Practising Dietitian (APD) before making changes, ideally in the context of a broader women’s health plan that might also explore support for polycystic ovary syndrome or endometriosis.
What is creatine? Basics, food sources and how it works
Creatine is a compound your body makes from three amino acids: arginine, glycine and methionine. Most of this happens in the liver and kidneys, with some in the brain, and then creatine travels through the blood into your muscles and other tissues (Kreider et al., 2017). About 90 – 95% of the body’s creatine lives in skeletal muscle, with smaller but important amounts in the brain and heart (Persky & Rawson, 2007). For a general overview of creatine’s discovery, metabolism and roles beyond sport, summaries such as this encyclopaedia-style review and historical analyses of creatine’s early trials provide useful background.
You also get creatine from food, mainly animal products like beef, pork and fish. That means vegetarians and vegans usually take in far less creatine from their diet. Over time, lower intake can add up, especially when combined with lower muscle mass, which is common in women. Your body still makes creatine, but diet can top up the tank when intake is adequate (Rawson & Volek, 2003).
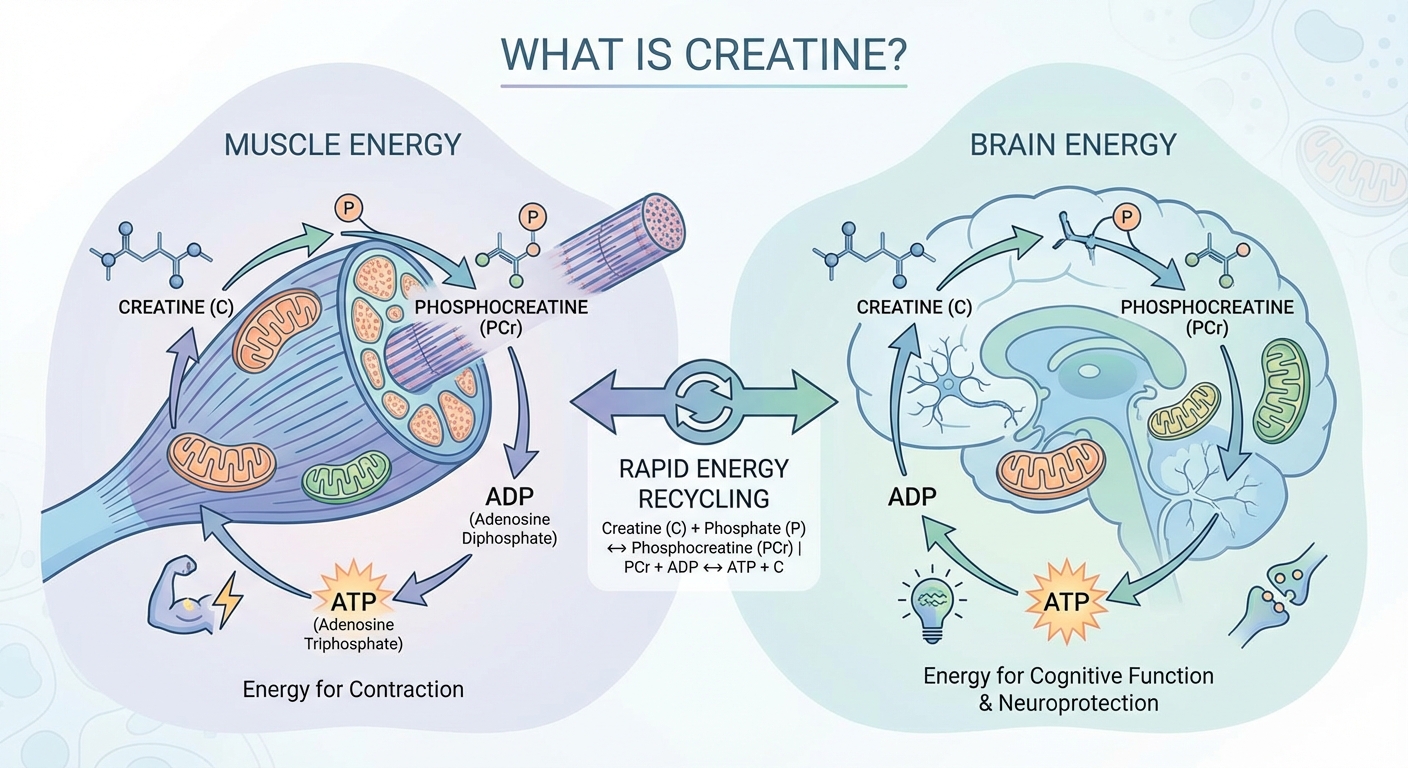
Why does your body bother with creatine at all? The short answer is: fast energy. Inside your cells, creatine and its partner phosphocreatine form a “phosphagen system”. This system helps recycle ATP, the main chemical your cells use for energy, especially when you suddenly need power – think sprinting to catch a bus or lifting a heavy shopping bag. Without enough creatine, that rapid energy system has less buffer to draw on (Allen, 2012).
The brain also uses creatine. Nerve cells need stable energy supply to keep you thinking clearly, managing mood, and reacting quickly. That is one reason researchers are now exploring creatine for brain fog, mental fatigue and neuroprotection, not just biceps and gym performance (Avgerinos et al., 2018). Popular summaries aimed at women highlight these emerging brain and mood benefits across the lifespan, including menopause, and discuss them in more detail than traditional sports-focused resources (lifespan reviews of creatine in women’s health; menopause-focused overviews).
Who traditionally used creatine and why is this shifting?
Creatine became popular in the 1990s as a sports supplement. The classic user was a young man in the gym chasing strength and size. Early studies focused almost entirely on male strength and power athletes – bodybuilders, sprinters and players in team sports like rugby or AFL – because those groups were easy to recruit and performance changes were simple to measure (Kreider et al., 2017). https://jissn.biomedcentral.com/articles/10.1186/s12970-017-0173-z
Marketing followed the research. For years, creatine tubs showed muscular men, heavy weights and explosive training imagery. Women were under-represented in trials, and many were told (often without evidence) that creatine was “too hardcore”, “bulking”, or only for high-level male athletes. It is not surprising that many women still feel unsure whether creatine is “for them”.
Over the last 10 – 15 years, the research base has broadened. Large reviews now show creatine can improve high-intensity performance and muscle function in a wide range of people, including older adults and clinical groups with muscle weakness or fatigue (Candow et al., 2014). At the same time, scientists started noticing something else: creatine is active in the brain, bones and other tissues, not just muscle.
This opened the door to a more nuanced question: if creatine biology is different in men and women, do women have unique needs across the life course? The 2025 paper “Creatine in women’s health: bridging the gap from menstruation through pregnancy to menopause” by Smith-Ryan and colleagues takes that question seriously and brings women’s health – not just sports performance – into the centre of the creatine conversation (Smith-Ryan et al., 2025). https://doi.org/10.1080/15502783.2025.2502094
In short, creatine has moved from a niche sports aid for young men to a potential tool for broader energy support, brain health and healthy ageing. The evidence is still growing, especially for women, but the old stereotype of creatine as “only for bodybuilders” is increasingly out of date. Accessible summaries written for women, including clinical reviews on creatine in menopause and beyond and integrative gynaecology perspectives on creatine for women’s health, reflect this shift in focus.
Sex differences in creatine biology, hormones and diet
One of the most important shifts in thinking is this: women are not just “smaller men” when it comes to creatine. Several reviews highlight key sex-specific differences in how creatine is made, stored and used across the body (Brosnan & Brosnan, 2016). Women generally have less total muscle mass than men, so they simply have less overall storage space for creatine. On top of that, there is evidence that women synthesise around 70 – 80% less creatine internally than men, which may lower baseline levels even further (Brosnan & Brosnan, 2016). https://doi.org/10.1093/nutrition/nuw021
Diet patterns also matter. Many women eat less red meat and fish than men, sometimes for cost, taste, or ethical reasons. That means lower dietary creatine intake, particularly in vegetarians and vegans. When you put these pieces together – less muscle, lower internal production, and often less intake – it is unsurprising that typical creatine levels may be lower in women. This does not mean every woman is deficient, but it does suggest that “average male data” may not tell the full story for female bodies.
Hormones add another layer. Oestrogen and progesterone, which rise and fall across the menstrual cycle and through life, appear to influence creatine metabolism and how energy is handled in tissues like muscle and brain (Ellery et al., 2016). During low-oestrogen phases, such as the late luteal phase or early menopause, some women experience more fatigue, mood changes and brain fog. Researchers now suspect changes in high-energy phosphate systems like the creatine – phosphocreatine system may contribute to these symptoms for some women (Smith-Ryan et al., 2025). https://doi.org/10.1080/15502783.2025.2502094
There is a catch, though. Current studies do not fully explain how creatine interacts with hormones such as oestrogen and progesterone across perimenopause or the menstrual cycle. We do not yet have reliable biomarkers that predict who will respond best, nor clear guidance for women with hormone-sensitive conditions. In many areas, clinicians still have to extrapolate from general creatine research rather than hormone-specific trials.
For now, the key message is nuance. Female sex, hormone status, diet, muscle mass and life stage all shape creatine needs. That is why conversations about creatine in women’s health should be individual, not one-size-fits-all, and ideally embedded within broader nutrition and women’s health services that consider your full medical and hormonal history.
Creatine across the female lifespan: menstruation, pregnancy and menopause
The 2025 article “Creatine in women’s health: bridging the gap from menstruation through pregnancy to menopause” pulls together emerging evidence on how creatine needs and benefits may shift across the female reproductive lifespan (Smith-Ryan et al., 2025). During menstruation and the menstrual cycle, fluctuating oestrogen and progesterone levels affect creatine synthesis and high-energy phosphate metabolism. Some early work suggests creatine could support performance, mood, and fatigue particularly during lower-oestrogen phases, though data are still limited. https://doi.org/10.1080/15502783.2025.2502094
In pregnancy, the focus is different. Pregnancy is an enormous metabolic task; both mother and fetus draw heavily on energy systems. Animal data and mechanistic human work suggest creatine stores in the placenta and foetal tissues may protect against low-oxygen episodes and energy stress (Ellery et al., 2016). There is interest in whether optimising maternal creatine status could support resilience during birth and complications such as preterm delivery or birth asphyxia, but high-quality human trials are sparse.
Postpartum, many women face sleep deprivation, low energy, and mood vulnerability. Theoretically, boosting creatine availability could help cells cope with repeated short-sleep cycles by supporting ATP production and buffering against fatigue. Reviews discuss this as a promising idea, especially for brain function in sleep-deprived new mothers, but here again, firm clinical evidence in humans is not yet available. That means any use in pregnancy or breastfeeding should only occur under medical supervision after weighing up potential risks and benefits with your obstetric team.
Later in life, during perimenopause and postmenopause, creatine research is more developed. Trials in midlife and older women suggest creatine, when combined with resistance training, can support muscle strength, lean mass and physical function, which are critical for falls prevention and independence (Candow et al., 2014). Small studies also hint at potential benefits for mood and cognition, but sample sizes are modest and follow-up is short, often less than eight weeks.
Across all stages, the pattern is similar: strong theoretical reasons to consider creatine, some encouraging early data, but clear gaps. Women-specific, long-term studies – not just short trials adapted from male sport science – are urgently needed. Until then, any decision to use creatine should be made with your GP or APD, taking into account pregnancy plans, hormone therapy, and your overall health picture, ideally as part of a comprehensive approach that also looks at fertility and preconception nutrition and pregnancy and postpartum care.
Benefits, risks and safety of creatine in women’s health

For the general adult population, creatine monohydrate is one of the most studied supplements, with a robust safety profile when used at typical intakes (Kreider et al., 2017). In women, short-term trials in contexts such as athletic performance, perimenopause and ageing support that creatine is usually well tolerated. Reported side effects are mostly mild – things like temporary bloating or stomach upset – and often related to high single doses or poor timing around meals. Long-term data in midlife and older women, however, are still limited.
When it works, what does creatine do? In sport, it consistently improves high-intensity exercise capacity, sprint performance, and gains in lean muscle when combined with resistance training. For women who strength train or play stop – start sports, these gains can translate into better training quality, more muscle protection, and potentially lower injury risk. Outside the gym, creatine’s support for muscle and bone strength may help with daily tasks such as climbing stairs, lifting children or carrying groceries, especially as we age (Candow et al., 2014).
For the brain, evidence suggests creatine may support short-term memory, reasoning and mental fatigue, particularly under stressors like sleep deprivation or complex cognitive tasks (Avgerinos et al., 2018). These brain effects are one reason some women are curious about creatine for brain fog in perimenopause, high-stress jobs, or new parenthood. Individual responses vary, so many clinicians encourage women to frame creatine as one optional tool within broader nutrition and lifestyle interventions rather than a stand-alone solution.
Risks are often overstated online. Concerns about kidney damage in healthy people using standard creatine intakes have not been supported by well-designed studies, although people with existing kidney disease or significant medical conditions should be more cautious and seek specialist advice before use (Poortmans & Francaux, 2000). Some individuals notice digestive upset or a subtle “wired” feeling if they take creatine late in the day, which may interfere with sleep onset. Because systematic studies on sleep and creatine are lacking, a simple precaution is to take it earlier in the day and monitor how you feel.
The bottom line: creatine appears safe for many women when used responsibly, but we lack long-term, women-specific trials, especially in pregnancy, breastfeeding and complex medical conditions. Any move from “nice idea” to “daily habit” should involve your GP or APD, particularly if you take multiple medicines or have hormone-sensitive conditions.
Why creatine quality matters: German Creapure and product choices
Not all creatine products are created equal. The form used in almost all research is creatine monohydrate – it is stable, well absorbed, and cost-effective. When you are reading studies showing benefits for strength, performance or brain health, they are almost always talking about this form, not fancy blends or novel salts (Kreider et al., 2017). From a clinical dietitian’s perspective, sticking close to the form used in trials makes sense if you want predictable results. https://jissn.biomedcentral.com/articles/10.1186/s12970-017-0173-z
Within creatine monohydrate, quality and purity still vary. Creapure is a branded form of creatine monohydrate manufactured in Germany under strict quality control, with tight limits on contaminants and by-products. Independent testing has repeatedly shown high purity, which is why many sports dietitians and medical teams prefer it when they can access it. For women who are already juggling medications, hormones and other supplements, reducing unnecessary exposure to impurities is a sensible priority.
Why emphasise purity so much? Creatine is usually taken daily over long periods. Even tiny amounts of unwanted compounds can add up over years if manufacturing is sloppy. Reputable brands using Creapure or equivalent quality-assured raw materials usually provide batch testing certificates and clear labelling. This level of transparency allows clinicians to feel more confident recommending a specific product when appropriate.
Practical checks when choosing a creatine product include:
- Looking for “creatine monohydrate” as the only active ingredient, rather than complex blends.
- Checking for quality marks such as Creapure branding or independent third-party testing.
- Avoiding products with many stimulants added, which can cloud whether any sleep or mood changes relate to creatine or caffeine.
- Choosing Australian-compliant supplements that meet local labelling and safety standards (Therapeutic Goods Administration guidance can help here). https://www.tga.gov.au
Even with a high-purity product, creatine is not a magic bullet. It is a tool that works best alongside the foundations: a balanced diet, enough protein, regular movement, sleep support, and appropriate medical care. Quality matters, but context matters just as much, which is why many women benefit from individualised guidance through dedicated women’s nutrition clinics that understand both supplements and broader health.
Practical tips: how to discuss creatine with your care team
If you are wondering whether creatine might fit into your health plan, start with a clear conversation with your GP or APD. Bring a short list of your goals – for example, “support strength and bone health in perimenopause”, “help manage fatigue during shift work”, or “explore options for brain fog”. Clear goals make it easier for your clinician to weigh up if creatine is relevant for you personally.
Before the appointment, write down:
- All medications and supplements you currently use, including over-the-counter products.
- Any kidney, liver, or hormone-related diagnoses.
- Pregnancy plans, breastfeeding status, or use of hormone therapy.
- Typical diet patterns (e.g., vegetarian, low red meat intake).
In the consult, you might ask:
- “Based on my health history, do you see any red flags for creatine?”
- “If we trial creatine, what should we monitor – blood tests, symptoms, or something else?”
- “How should creatine fit with my exercise program, especially resistance training?”
Your clinician may suggest monitoring kidney function or adjusting use around surgery, pregnancy or new medications. They may also help you choose a high-quality product and discuss general intake patterns and timing that suit your lifestyle, while avoiding exact dose instructions on public information sheets. If creatine is not right for you, they can help you explore other strategies for energy, mood and strength that better match your situation, such as working with a team experienced in fertility and preconception nutrition or pregnancy and postpartum recovery.
Conclusion and next steps
Creatine is far more than a gym supplement. It is a core energy molecule with roles in muscle, brain, and possibly reproductive health – and women have been missing from the story for too long. Newer research, including the 2025 review on creatine in women’s health, suggests that life stage, hormones, diet and muscle mass all shape how creatine behaves in female bodies.
At the same time, there are still big gaps: limited pregnancy and postpartum data, short trial durations, and unanswered questions about who benefits most. If you are curious about creatine for strength, brain fog or healthy ageing, your next step is a personalised discussion with your GP or an Accredited Practising Dietitian. They can help you decide whether a high-quality creatine monohydrate product fits safely into your broader plan – or whether other strategies should come first. If you would like a practitioner team that regularly works with hormonal conditions, learn more about Ausclin’s women’s health focus or touch base via their introductory resources, including their blog and updates page; if you ever land on a page-not-found link, try navigating back to the main services menu.

References and search strategy
Search strategy (17 February 2026)
Databases searched: PubMed, Google Scholar. Key terms included: “creatine women’s health”, “creatine menstruation menopause pregnancy”, “sex differences creatine metabolism”, “creatine monohydrate safety”, “creatine brain health”, “creatine sleep effects”. Filters: human where available, English language, emphasis on publications from 2010 – 2025 plus key earlier foundational papers. Australian regulatory information was sourced from the Therapeutic Goods Administration, and consumer-focused explanations were cross-checked against expert summaries on creatine and healthy ageing in women and historical perspectives on creatine powder.
Key references
- Smith-Ryan, A. E., DelBiondo, G. M., Brown, A. F., Kleiner, S. M., Tran, N. T., & Ellery, S. J. (2025). Creatine in women’s health: Bridging the gap from menstruation through pregnancy to menopause. Journal of the International Society of Sports Nutrition. Advance online publication. https://doi.org/10.1080/15502783.2025.2502094
- Kreider, R. B., Kalman, D. S., Antonio, J., et al. (2017). International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition, 14(1), 18. https://jissn.biomedcentral.com/articles/10.1186/s12970-017-0173-z
- Brosnan, J. T., & Brosnan, M. E. (2016). The role of dietary creatine. Nutrition Reviews, 74(11), 708 – 717. https://doi.org/10.1093/nutrit/nuw021
- Candow, D. G., Chilibeck, P. D., Forbes, S. C., et al. (2014). Factors influencing the effectiveness of creatine supplementation as a therapeutic intervention for sarcopenia. Frontiers in Nutrition, 1, 13. https://doi.org/10.3389/fnut.2014.00013
- Ellery, S. J., LaRosa, D. A., & Morrison, J. L. (2016). Placental creatine metabolism and transport in pregnancy. Placenta, 41, 22 – 28. https://doi.org/10.1016/j.placenta.2016.03.012
- Avgerinos, K. I., Spyrou, N., Bougioukas, K. I., & Kapogiannis, D. (2018). Effects of creatine supplementation on cognitive function of healthy individuals: A systematic review of randomized controlled trials. Experimental Gerontology, 108, 166 – 173. https://doi.org/10.1016/j.exger.2018.04.013
- Poortmans, J. R., & Francaux, M. (2000). Long-term oral creatine supplementation does not impair renal function in healthy athletes. Medicine & Science in Sports & Exercise, 32(12), 1106 – 1110. https://doi.org/10.1097/00005768-199912000-00020
- Therapeutic Goods Administration. (n.d.). Medicines and medical devices regulation. Retrieved 17 February 2026, from https://www.tga.gov.au
All content in this article is for general educational purposes only and does not constitute personalised medical, diagnostic or nutritional advice. Always consult your GP, treating specialist or an Accredited Practising Dietitian for individual guidance, ideally within a coordinated care plan such as those offered by specialised women’s health clinics like Ausclin.
Frequently Asked Questions
What is creatine and why is it important for women’s health?
Creatine is a naturally occurring compound made from amino acids that helps your cells rapidly produce energy, especially in muscles and the brain. For women, it may support strength, muscle maintenance, cognition, mood and healthy ageing across life stages, from menstruation through pregnancy to menopause. Because women often have lower muscle mass and may consume less dietary creatine (especially if vegetarian or vegan), supplementation can be particularly relevant. Always discuss supplementation with your GP or an Accredited Practising Dietitian (APD) before starting.
Is creatine safe for women to take during their period, pregnancy or menopause?
Current research, including the 2025 article “Creatine in women’s health: bridging the gap from menstruation through pregnancy to menopause,” suggests creatine is generally safe for healthy women when used at evidence-based doses. Emerging data indicate potential benefits in pregnancy and menopause, but studies are still limited, so individual medical advice is essential. Women with kidney disease, significant medical conditions or those on medication should only use creatine under professional supervision. Always consult your GP, obstetrician or APD before using creatine in pregnancy or if you’re perimenopausal or postmenopausal.
Does creatine make women gain weight or look bulky?
Creatine can cause a small increase in body weight due to more water being stored inside the muscle, not because of fat gain. In women, this usually translates to better muscle fullness and strength rather than a bulky or “puffy” look, especially at standard daily doses (3–5 g). The change is often modest and many women don’t notice it visually. If you’re concerned, an APD or sports dietitian can help tailor dose and timing around your goals.
What are the benefits of creatine for women who don’t play sports or go to the gym?
Creatine isn’t just for athletes; it supports energy in every cell, including the brain. Early research in women suggests possible benefits for cognitive function, mood, fatigue and maintaining muscle as you age, even if you’re not training intensely. It may be particularly useful during life stages with higher energy demand or hormonal change, like pregnancy and menopause. However, it should sit within a broader health plan that also addresses diet, sleep, movement and any conditions like PCOS or endometriosis.
What is Creapure and why do people say German creatine is better?
Creapure is a branded form of creatine monohydrate manufactured in Germany, known for high purity and strict quality control. It is tested for contaminants such as heavy metals and unwanted by-products, which can be an issue with lower‑quality creatine from less regulated facilities. For many women, especially those pregnant, planning pregnancy or managing chronic conditions, choosing a high‑purity product is a simple way to reduce unnecessary risk. AusClin recommends using reputable, tested creatine sources such as Creapure as part of a medically guided plan.
How much creatine should women take per day and do they need a loading phase?
Most research in adults, including women, uses 3–5 g of creatine monohydrate per day, taken consistently. A loading phase (about 20 g per day split into 4 doses for 5–7 days) can saturate muscles faster, but it’s not essential and some women prefer to skip it to reduce the chance of mild bloating. Over a few weeks, daily low-dose use reaches similar muscle creatine levels. Your ideal approach depends on your health status and goals, so check with an APD or clinician before starting.
What are the risks or side effects of creatine for women?
In healthy adults, creatine monohydrate is one of the most studied supplements and is generally well tolerated, with the most common side effects being mild bloating or stomach upset, especially if large doses are taken at once. Concerns about kidney damage have not been supported by research in people with normal kidney function using standard doses. Women with kidney disease, high blood pressure, pregnancy complications or those on certain medications should be assessed individually before using creatine. Using a pure product like Creapure, staying hydrated and following evidence-based dosing can help minimise risks.
Is creatine good for vegetarian or vegan women?
Yes, creatine can be particularly useful for vegetarian and vegan women because plant-based diets contain little to no creatine from food. Studies show that people with lower baseline creatine levels often respond more strongly to supplementation, with greater improvements in strength, performance and sometimes cognition. A standard 3–5 g daily dose of creatine monohydrate is typically used in research. Discuss this with a dietitian who understands plant-based nutrition to fit creatine into your overall nutrient plan.
Can creatine help women with conditions like PCOS or endometriosis?
Creatine is not a direct treatment for PCOS or endometriosis, but by supporting muscle mass, energy metabolism and possibly mood and cognition, it may complement broader management strategies. Women with chronic pain, fatigue or exercise limitations from these conditions may find creatine helps them tolerate and benefit more from resistance training and physical activity. Because hormones, inflammation and medications can be involved, supplement decisions should be made with a GP, gynaecologist or APD. AusClin clinicians can help integrate creatine into a personalised women’s health plan if it’s appropriate.
Where can I get guidance on whether creatine is right for my stage of life?
The safest approach is to discuss creatine with a health professional who understands both supplements and women’s health across the lifespan. At AusClin, doctors and Accredited Practising Dietitians can review your menstrual history, pregnancy plans, perimenopause/menopause status and any conditions like PCOS or endometriosis before making a recommendation. They can also help you select a high‑quality product (such as Creapure-based creatine), set a suitable dose and monitor your response over time. This ensures creatine is used as part of a comprehensive, evidence‑based care plan.