
Date published: 27 February 2026
Estimated reading time: 13 minutes
GLP-1 medications have changed the way many Australians think about weight, appetite and food. These drugs can quiet constant “food noise”, reduce hunger and support weight and diabetes management, but they also change how you eat, and sometimes how you feel about eating at all. That’s why nutrition, micronutrients, protein, muscle and your relationship with food all matter just as much as the injection itself.
We look at what GLP-1 (and dual GIP/GLP‑1) medications do in the body, the real risks of missing key vitamins, minerals and protein, and how to protect your muscles while losing weight, drawing on guidance from clinical nutrition programs for GLP‑1 users.
All content here is for general education only. It is not personalised medical, diagnostic or nutrition advice. Always speak with your GP, specialist or an Accredited Practising Dietitian (APD) before making changes to your medication, diet or supplements, and consider working with an APD who understands Australian GLP‑1 nutrition care.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9994304/ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10107620/
Micronutrient Risk on GLP-1 Medications
GLP‑1 receptor agonists like semaglutide and dual GIP/GLP‑1 drugs like tirzepatide slow stomach emptying and reduce appetite. Food sits in the stomach for longer, and people feel full after only a few bites. Many go from three meals and snacks to one or two small meals a day without planning it. This rapid drop in food volume is where micronutrient risk starts: the problem is not the drug alone, but the combination of less food and less variety, which is why recent narrative reviews of dietary intake on GLP‑1 and GIP/GLP‑1 therapies are calling for closer nutrition monitoring.
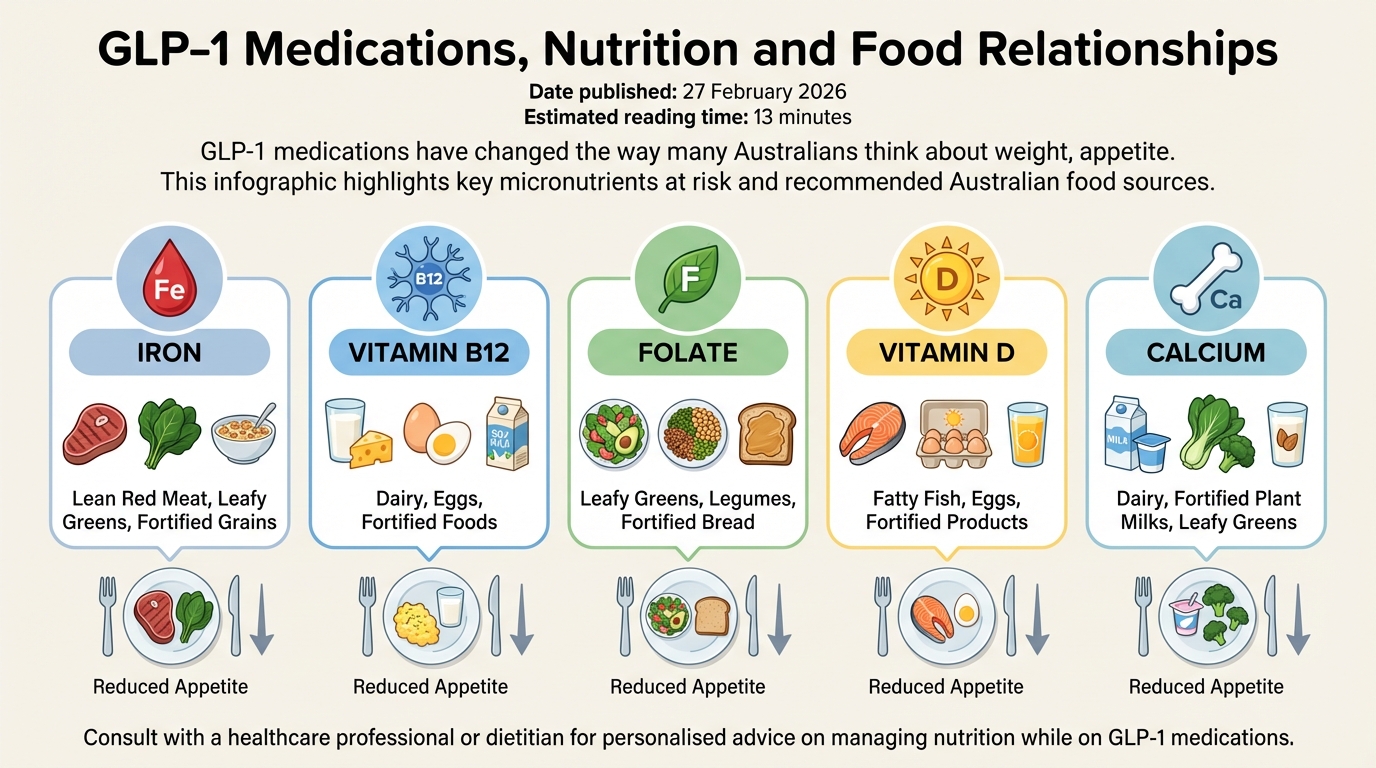
When intake shrinks, it becomes harder to reach daily needs for vitamins and minerals. Iron, vitamin B12, folate, vitamin D and calcium are often the first to slip, especially if meat, dairy or fortified grains are reduced due to nausea or food aversion. In Australia, iron deficiency is already common in people who menstruate, so adding GLP‑1‑related appetite loss can quietly push levels down further, sometimes without obvious symptoms until you’re quite low. Many GLP‑1 clients at dietitian‑led nutrition services need tailored micronutrient checks.
Gastrointestinal side effects such as nausea, vomiting and diarrhoea can magnify this. Some people start avoiding red meat, salad, whole grains or dairy because they “feel heavy” or seem to trigger queasiness. Over time that can mean less iron, less B12, less fibre and fewer antioxidants on the plate. Research reviews show clear reductions in total kilojoule intake on GLP‑1s, but the pattern of which foods fall away is highly individual, so you cannot assume you are safe just because your bloods looked fine a year ago; expert groups now highlight that nutritional priorities need to be built into GLP‑1 obesity care.
Because therapeutic supplement doses can carry risks, especially alongside other medicines, decisions about blood tests and supplementation should be made with your GP or APD. They can check for low ferritin, B12, folate and vitamin D, and suggest food-based strategies first, then supplements if needed, often as part of a broader life‑stage and pregnancy/postpartum nutrition plan where relevant.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10486563/ https://www.health.gov.au/resources/publications/australian-dietary-guidelines
Protein Intake and Muscle Preservation on GLP-1s

Weight loss from GLP‑1 medications is not just fat. Without enough protein and resistance-style movement, you can also lose lean mass, including muscle. Clinical trials of GLP‑1 and GIP/GLP‑1 therapies show meaningful total weight loss, but a slice of that loss comes from fat‑free mass (which includes muscle, bone and body water) (Jendle et al., 2022). Losing some lean tissue is expected in any energy deficit. The goal is to protect as much muscle and bone as possible while still allowing fat loss, something that structured preconception and metabolic nutrition support can help with.
Lower appetite makes this balancing act trickier. Many people on GLP‑1s feel satisfied with a few crackers, a coffee or a couple of forkfuls of dinner. Those small “snack-like” intakes often lack solid protein sources such as eggs, yoghurt, legumes, tofu, fish or lean meats. Over weeks and months, daily protein can fall well below what your body needs to maintain muscle, especially if you already have lower muscle mass, are over 50, or live with chronic illness; clinicians are increasingly emphasising protein planning in GLP‑1 diets, as reflected in practical GLP‑1 diet guidance from major health centres.
A useful way to think about it is this: if your total food volume has halved, the protein density of what you do eat needs to almost double. That usually means anchoring each meal or snack around a protein source, then building plants (vegetables, fruit, whole grains, nuts, seeds) around it. For example, instead of just soup, you might choose lentil and vegetable soup with grated cheese; instead of toast alone, baked beans on grainy toast with avocado – strategies dietitians routinely weave into chronic condition meal plans.
Resistance training – anything that makes muscles work against load, like body‑weight exercises, resistance bands or weights – also helps signal the body to preserve muscle while you lose fat. Even two short sessions a week can make a meaningful difference. This does not need to be a gym membership; an APD working closely with your GP or physiotherapist can help you match food and movement to your energy levels and medical history, in the same way they would for clients managing polycystic ovary syndrome alongside GLP‑1 therapy.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10552824/ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6342899/
The Role of Dietitians in GLP-1 Nutrition, Side-Effect Management and Food Relationships

Many people stop GLP‑1 medications early because of side effects, unrealistic expectations or feeling unsure how to eat on them. This is where an Accredited Practising Dietitian can change the whole trajectory. Dietitians help you build a structured, nutrient‑dense, lower‑volume eating pattern that fits your appetite, culture, budget and health conditions, rather than leaving you to live on dry crackers and hope for the best, and organisations experienced in GLP‑1 care, such as Ausclin, integrate this support into routine consultations.
Dietitian‑led care often focuses on three core areas. First, side‑effect management: tactics such as smaller, more frequent meals, choosing softer textures, careful fat intake, adding ginger or peppermint, and clear hydration plans can reduce nausea, bloating and constipation for many people. Second, micronutrient protection: APDs can review your usual intake, medical history and blood tests, then suggest targeted food swaps and, if needed, supplements under medical supervision. Third, long‑term behaviour change: small, steady habit shifts you can continue after the injections stop; professional bodies now highlight that working with a dietitian can maximise GLP‑1 results and protect nutrition in diabetes care. Studies comparing medication‑only care to programs that combine GLP‑1 therapy with nutrition and behavioural support show better sustained weight loss, fewer side effects and less weight regain once the drug is stopped in the supported groups (Wilding et al., 2021).
For people with complex medical needs – such as type 2 diabetes, kidney disease, gastrointestinal conditions or a history of bariatric surgery – working with an APD is even more important. They can coordinate with your GP and treating specialists, adjust advice as medications change, and watch for red flags like rapid weight loss, disordered eating patterns, or signs of malnutrition that might be missed in a quick consult; questions about how GLP‑1 drugs are changing dietetics practice more broadly are also being explored in emerging commentaries on how GLP‑1 medications are affecting dietetic care.
Many people describe GLP‑1 medications as finally “turning down the volume” on food thoughts. Constant cravings, binge episodes and late‑night grazing can ease, which often brings a huge sense of relief. Appetite suppression can sometimes mask disordered eating. Skipping meals, ignoring hunger cues, feeling anxious about social meals, or taking pride in how little you can eat may be praised in diet culture, but they can signal that your relationship with food is becoming more rigid, not healthier, making access to weight‑neutral, food-relationship‑focused nutrition support particularly valuable.
Dietitians trained in non‑diet and intuitive eating approaches can help you use the “quieter” appetite window to build more balanced patterns instead of stricter rules. That might include scheduling regular meals even when you are not very hungry, keeping favourite foods in your plan without labelling them as “bad”, learning to notice early signs that you are under‑fuelling, and practising flexible thinking around eating out, travel and celebrations. Screening for eating disorders is also key. If you have a current or past history of anorexia, bulimia, binge eating disorder or other disordered patterns, it is vital that your GLP‑1 therapy is co‑managed with your mental health team and an APD experienced in this space, supported by resources such as the InsideOut Institute.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10292139/ https://www.racgp.org.au/clinical-resources/clinical-guidelines/key-racgp-guidelines/view-all-racgp-guidelines/obesity https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11208099/
Practical Tips and Next Steps

Turning the science into daily habits is where most people need clear, simple ideas. While your exact plan should be tailored with your healthcare team, a few broad principles tend to help many GLP‑1 users.
Aim for three small, protein‑focused eating occasions each day, even if your appetite is low. This might look like yoghurt with nuts and berries, a half‑sandwich with chicken and salad, or lentil soup with toast. When only 50 – 60% of your former food volume fits, each bite needs to work harder: colourful vegetables, fruit, whole grains, legumes, nuts, seeds, and quality proteins become the backbone of your meals, a pattern echoed in clinical advice that nutrition is vital when using GLP‑1 weight‑loss medications.
Drink regularly across the day can reduce constipation and help manage nausea. Notice patterns that worsen side effects, large, greasy dinners, fizzy drinks, lying flat right after eating – and experiment with changes like smaller portions, softer textures or earlier mealtimes. Build in regular reviews of your blood tests and symptoms with your GP and an APD so micronutrient or muscle issues can be picked up early rather than years down the track, something that structured pregnancy and postpartum nutrition reviews already model well.
GLP‑1 medications can be powerful tools for managing type 2 diabetes and reducing weight, but they reshape much more than your appetite. They shift your micronutrient intake, protein needs, muscle balance and relationship with food. With structured, nutrient‑dense eating, enough protein, resistance‑style movement and skilled dietetic support, you can tilt those changes towards better health instead of hidden deficits and fragile eating patterns, and clinics like Ausclin are designed to support this kind of joined‑up care.
Whether you are navigating perimenopause or menopause, managing insulin resistance or prediabetes due to a complex history of PCOS, or using GLP-1 medications as part of your health journey, nutrition plays a foundational role. Attention to micronutrients, protein intake, and food relationships helps protect iron status, muscle and bone health, and long-term wellbeing. Dietitian support can provide personalised guidance so your nutrition plan aligns with your medical care and life stage goals, helping you achieve sustainable results without compromising overall health.
If you are already using a GLP‑1 medication, or your GP is considering one, speak with your healthcare team about a referral to an Accredited Practising Dietitian experienced in this area.
Remember, this information is general only. Do not change your medication, supplements or eating plan based on an article; always discuss specific decisions with your own healthcare team, who know your medical history and can guide you safely. None of the GLP-1 RAs should be used during pregnancy and individuals of childbearing potential are advised to use effective contraception.
https://www.health.gov.au/resources/publications/australian-dietary-guidelines https://www.nrv.gov.au/
References and Search Strategy
Evidence for this article was sourced on 25 February 2026 using PubMed, Google Scholar and Australian government and guideline sites. Key search terms included “GLP‑1 receptor agonist nutrition”, “tirzepatide dietary intake”, “GLP‑1 micronutrient deficiency”, “GLP‑1 lean mass loss”, “GLP‑1 food noise emotional eating”, “dietitian support GLP‑1 weight maintenance”, “Australian Dietary Guidelines” and “NHMRC Nutrient Reference Values”, alongside contemporary practice pieces such as nutrition plans for GLP‑1 medications and dietary recommendations for managing GLP‑1‑related gastrointestinal symptoms.
Key References
-
Jendle, J., Grunberger, G., Blevins, T., Giorgino, F., Hietpas, R. T., Botros, F. T., & Frias, J. P. (2022). Efficacy and safety of once‑weekly tirzepatide versus semaglutide in patients with type 2 diabetes (SURPASS‑2). New England Journal of Medicine, 385(6), 503 – 515. https://doi.org/10.1056/NEJMoa2107519
-
Wilding, J. P. H., Batterham, R. L., Calanna, S., Davies, M., Van Gaal, L. F., Lingvay, I., … Kushner, R. F. (2021). Once‑weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine, 384(11), 989 – 1002. https://doi.org/10.1056/NEJMoa2032183
-
Nauck, M. A., & Meier, J. J. (2019). Incretin hormones: Their role in health and disease. Diabetes, Obesity and Metabolism, 21(S1), 5 – 21. https://doi.org/10.1111/dom.13548
-
Rubino, D., Abrahamsson, N., Davies, M., Hesse, D., Greenway, F. L., Jensen, C., … Rosenstock, J. (2021). Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity. JAMA, 325(14), 1414 – 1425. https://doi.org/10.1001/jama.2021.1831
-
National Health and Medical Research Council. (2013). Australian Dietary Guidelines. Canberra: NHMRC. https://www.eatforhealth.gov.au/sites/default/files/content/The%20Guidelines/n55_australian_dietary_guidelines.pdf
-
National Health and Medical Research Council. (2017). Nutrient Reference Values for Australia and New Zealand. https://www.nrv.gov.au/
-
RACGP. (2019). Management of obesity. In: Guidelines for preventive activities in general practice. Royal Australian College of General Practitioners. https://www.racgp.org.au/clinical-resources/clinical-guidelines
-
Cucuzzella, M., & Haines, S. T. (2024). Weight management medications and the risk of disordered eating. Current Obesity Reports, 13, 1 – 12. https://doi.org/10.1007/s13679-024-00503-0
-
InsideOut Institute. (n.d.). Eating disorders information and resources. University of Sydney. https://www.insideoutinstitute.org.au/
This article is for general educational purposes only and is not a substitute for personalised medical or nutrition advice. Always consult your GP, treating specialist or an Accredited Practising Dietitian for individual guidance.
Frequently Asked Questions
What do GLP-1 medications like Ozempic and Mounjaro actually do to your appetite and eating habits?
GLP-1 and dual GIP/GLP-1 medications work by slowing stomach emptying and acting on appetite centres in the brain, so you feel full sooner and stay full for longer. Many people naturally move from three meals plus snacks to one or two small meals without planning to, which can dramatically change how much and how often they eat.
Can GLP-1 weight loss medications cause vitamin or mineral deficiencies?
Yes, GLP-1 medications can increase micronutrient risk because you’re eating less total food and often less variety, not because the drug directly “removes” nutrients. This can make it harder to meet needs for nutrients like iron, B12, folate, calcium and vitamin D, especially if you already had a low intake or follow a restrictive diet, so monitoring and targeted supplements may be needed.
How much protein should I eat when I’m on GLP-1 medication to protect my muscle?
Most adults on GLP-1 therapy benefit from aiming for roughly 1.2–1.6 g of protein per kg of body weight per day, split across meals, but your exact target should be set with a dietitian or doctor. Prioritising a high‑protein food at each eating occasion (for example eggs, Greek yoghurt, tofu, lean meat, fish or legumes) helps minimise muscle loss while you’re losing weight.
Do GLP-1 medications make you lose muscle as well as fat?
All forms of weight loss, including weight loss with GLP-1 medications, involve some loss of both fat mass and lean mass, including muscle. You can reduce the amount of muscle lost by keeping your protein intake up, doing regular resistance or strength training, and working with a dietitian to ensure your calorie deficit isn’t too extreme.
What should I eat in a day on GLP-1 medication if I get full after a few bites?
When your appetite is low, focus on small, nutrient‑dense meals rather than large plates of low-calorie foods. This usually means including a quality protein source, a healthy fat, and some colourful vegetables or fruit at each meal, and using snacks such as yoghurt, nuts, cheese, boiled eggs, or smoothies to top up protein and micronutrients if you can’t finish full meals.
How can an Accredited Practising Dietitian help me if I’m taking GLP-1 injections?
An Accredited Practising Dietitian (APD) can assess your current intake, tailor a meal plan that fits your reduced appetite, and help you meet protein and micronutrient needs while losing weight. At clinics like AusClin, dietitians also monitor for side effects, coordinate with your GP or specialist, advise on supplements where appropriate, and support you to keep a healthy relationship with food instead of slipping into overly restrictive patterns.
Do I need vitamin or mineral supplements when using GLP-1 meds, or is food enough?
Some people can meet their micronutrient needs with careful food choices, but many on GLP‑1 therapy need at least a basic multivitamin or targeted supplements, particularly if they have a low appetite or pre‑existing deficiencies. Blood tests ordered by your GP or specialist, interpreted with an APD, are the safest way to decide what to take rather than guessing or buying multiple over‑the‑counter products.
How can I stop GLP-1 medication from making my relationship with food worse?
Work on keeping regular, balanced meals instead of skipping eating altogether just because you’re not hungry, and avoid turning every bite into a strict calorie calculation. A dietitian experienced with GLP‑1 users, like those at AusClin, can help you challenge all‑or‑nothing thinking, reduce guilt around eating, and build flexible habits so food feels supportive rather than stressful while you’re on the medication.
Is it better to see a GP or a dietitian for nutrition advice while on GLP-1 injections?
Your GP or specialist is essential for prescribing and monitoring the medication, but they generally don’t have time to provide detailed, ongoing nutrition support. An Accredited Practising Dietitian complements your medical care by focusing on what, when and how you eat, tracking muscle and micronutrient status, and helping you develop sustainable habits so your results last after the injections stop.
What should I do if I feel no interest in food at all while taking GLP-1 medication?
If your interest in food disappears, first discuss this with your prescribing doctor to rule out excessive dosing or other medical issues. In parallel, a dietitian can help you set up simple, structured eating times, use easy‑to‑tolerate foods (like smoothies, soups and soft proteins), and ensure you still meet minimum energy, protein and micronutrient needs despite low appetite.