
Date published: 04 March 2026
Estimated reading time: 15 – 18 minutes
Endometriosis dietitian support: how nutrition can help during Endometriosis Awareness Month
Endometriosis Awareness Month is a powerful reminder that pain, bloating and fatigue are not “just part of being a woman”. Alongside surgery, medications and physical therapies, working with an endometriosis dietitian is an often-overlooked way to support hormone balance, inflammation, gut health and day-to-day quality of life.
An experienced endometriosis dietitian uses medical nutrition therapy to help reduce pelvic pain, manage fatigue, support bowel regularity and optimise micronutrient intake. This might include structured dietary changes, targeted fibre strategies to help bind and excrete estrogen, and careful use of supplements where needed, always tailored to your symptoms, medical history and lifestyle.
This article explains how nutrition fits into endometriosis care in Australia, and how clinics such as Ausclin integrate dietetic support into broader care. We will look at:
-
Why a dietitian is different from general nutrition advice
-
How fibre and gut health affect estrogen metabolism
-
Anti-inflammatory patterns such as the Mediterranean diet
-
Using low FODMAP and other targeted diets safely
-
Key micronutrients and emerging options like ketogenic or MCT-modified diets
-
How to find and work with an Accredited Practising Dietitian (APD)
All content here is for general education only and does not replace individual medical or dietetic advice. Always discuss changes with your GP, gynaecologist or APD.
What is endometriosis and why see a dietitian?
Endometriosis is a chronic, estrogen-dependent inflammatory condition where tissue similar to the lining of the uterus grows outside the uterus. It can cause pelvic pain, painful periods, pain with sex or bowel movements, bloating, fatigue and fertility problems. Symptoms often impact work, relationships and mental health over many years.
In Australia, gynaecologists lead diagnosis and medical or surgical management, but endometriosis does not exist in a vacuum: it interacts with digestion, immune function, stress and sleep. That is where a dietitian comes in. An endometriosis dietitian looks at how food choices can modulate inflammation, support hormone metabolism, stabilise energy and improve bowel patterns, while also preventing nutrient deficiencies.
Research suggests that structured, dietitian-guided nutrition plans lead to better symptom control than self-managed dietary changes or medication alone, with around 60% of women improving on targeted diets compared with 26% in control groups (https://pubmed.ncbi.nlm.nih.gov). Diet is not a cure, and it does not replace hormonal therapy, surgery or pain medication, but it can be a potent “add-on” that helps people cope between flares and after surgery. Reviews of dietary interventions in endometriosis consistently highlight the value of medical nutrition therapy in symptom management across a range of dietary patterns.
An Accredited Practising Dietitian can also help you navigate the sea of online advice. Many people with endometriosis experiment with gluten-free, dairy-free, vegan, “anti-inflammatory” or very low-carbohydrate diets without guidance. Sometimes these shifts help, but they can also become overly restrictive, exhausting to maintain and nutritionally inadequate. A dietitian’s role is to personalise, simplify and safeguard by keeping what works, discarding what does not, and making sure your nutrition remains robust for the long term.
Evidence overview source: https://www.ncbi.nlm.nih.gov/pmc/
Medical nutrition therapy with an endometriosis dietitian
Medical nutrition therapy is a structured, evidence-based way of using food and nutrients to manage health conditions. For endometriosis, an APD will usually start with a comprehensive assessment: symptom patterns (pain, bloating, bowel changes), menstrual cycle features, medical and surgical history, medications, current diet, supplement use and lab results where available.
From there, they design an individualised plan that may target four main areas:
-
Inflammation: shifting overall dietary pattern toward anti-inflammatory foods and away from known pro-inflammatory fats and ultra-processed foods.
-
Estrogen metabolism: increasing particular types of fibre to support estrogen binding and excretion in the gut.
-
Gut function: addressing constipation, diarrhoea, bloating or IBS-like symptoms with strategies such as low FODMAP, gentle fibre titration and probiotic foods.
-
Micronutrient status: checking for and correcting gaps in vitamin D, iron, magnesium, zinc, antioxidants and others, using food first and supplements if clinically indicated.
Many dietitians work within multidisciplinary teams, communicating with your gynaecologist, pelvic physiotherapist and psychologist when appropriate. This “joined-up” approach means your dietary plan can be timed around surgeries, fertility treatments or medication changes, minimising clashes and maximising benefit.
Importantly, dietitian-guided interventions are time-limited and structured. A common framework is a 4 – 12 week trial of a specific dietary pattern (for example, a Mediterranean-style plan, or a low FODMAP protocol when gut symptoms are prominent), followed by systematic reintroduction and personalisation. This helps identify genuine triggers without leaving you stuck on a highly restrictive diet for years.
Clinical trials indicate that dietary changes guided by health professionals can improve pelvic pain, abdominal pain, bloating, fatigue and quality of life scores compared with usual care (https://doi.org/10.1016/j.rbmo.2019.08.007). However, response is highly individual; an APD monitors outcomes and adjusts strategies rather than assuming a one-size-fits-all “endometriosis diet” exists. Recent work on medical nutrition therapy for pelvic pain and endometriosis shows particular benefits when structured plans such as Mediterranean or modified ketogenic diets are implemented with professional oversight over several weeks to months.
Fibre, gut health and estrogen balance in endometriosis
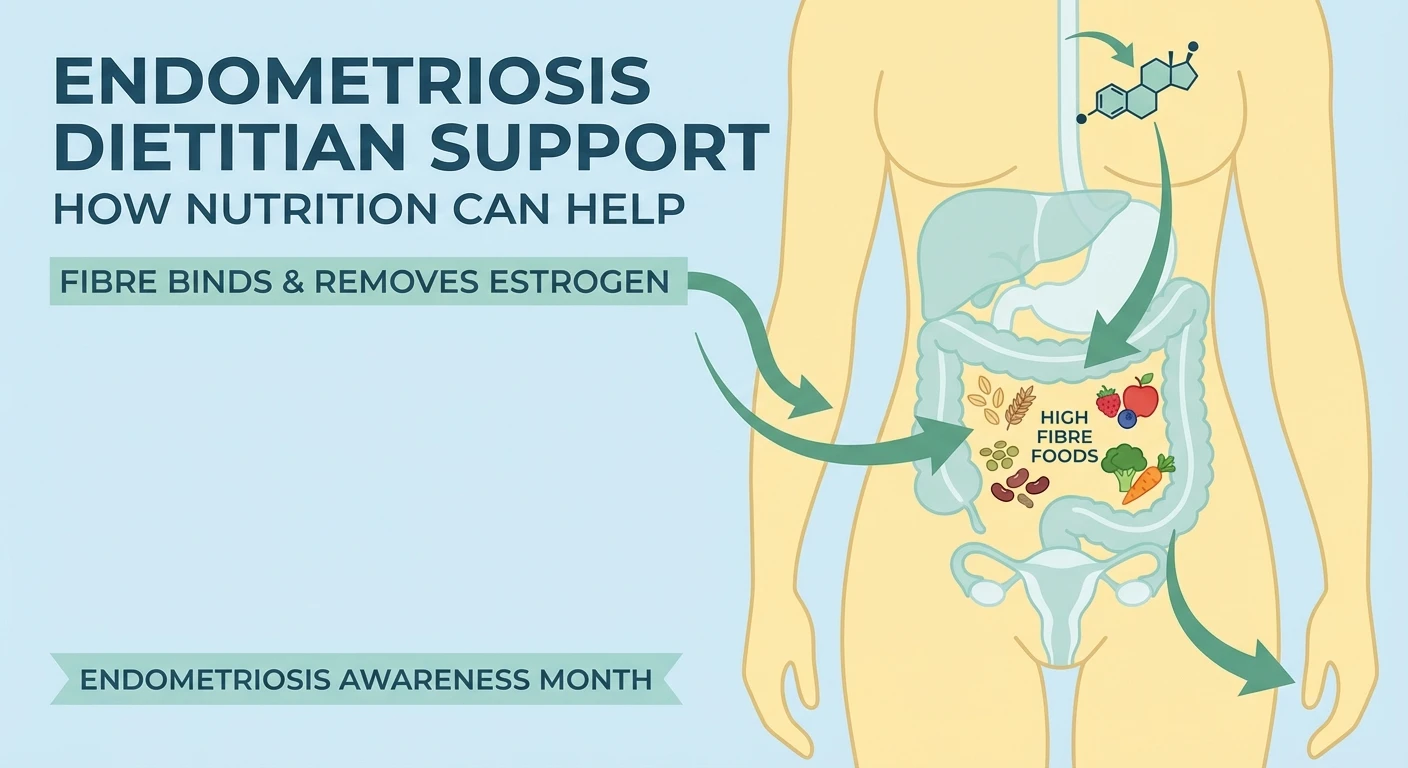
Endometriosis is strongly influenced by estrogen. While most estrogen is produced by the ovaries, the way your body processes and eliminates estrogen also matters. The liver packages estrogen so it can be excreted in bile, and the gut then plays a key role in getting it out of the body. This is where dietary fibre earns its place.
Certain fibres bind estrogen and its metabolites in the gut, helping carry them out in stool. Higher fibre intakes are associated with lower circulating estrogen levels, with some studies suggesting reductions in the range of 10 – 25% when fibre intake increases substantially (https://doi.org/10.1210/jcem-77-1-154). For someone with an estrogen-dependent condition, that shift may support other treatments aimed at suppressing or modulating hormones. Reviews of diet and endometriosis note that higher fibre, plant-forward patterns are consistently linked with more favourable hormone profiles and symptom trends across observational and interventional studies.
An endometriosis dietitian will usually focus on a variety of fibre types:
-
Insoluble fibre from whole grains, bran, nuts, seeds and many vegetables helps add bulk and speed transit, useful for constipation.
-
Soluble and gel-forming fibres from oats, barley, psyllium, legumes and some fruits help form soft, comfortable stools and can support blood glucose control.
-
Other plant compounds: Lignans from seeds like flaxseed (linseed) have weak phytoestrogenic activity and may support hormone balance in some people.
Clinically, the goal is not simply “more fibre at any cost” but “the right fibre, at the right pace”. Rapidly jumping from a low-fibre, ultra-processed pattern to a very high-fibre, legume-rich plan can worsen bloating and pain, especially if you also have IBS. An APD will usually increase fibre gradually, pair it with adequate fluids, and monitor your response.
Practically, a dietitian might help you build meals such as:
-
Oats cooked with milk/soy/ lactose-free milk, topped with ground flaxseed and berries
-
Wholegrain or legume-based pasta with tomato, vegetables, olive oil and grilled fish
-
Lentil or chickpea salad with leafy greens, pumpkin seeds and extra-virgin olive oil
Evidence summary source: https://doi.org/10.1210/jcem-77-1-154
Anti-inflammatory diet patterns and pain management in endometriosis
Chronic inflammation is a core feature of endometriosis. Immune cells around endometrial lesions release inflammatory mediators, which can sensitise nerves and amplify pain. Diet cannot “switch off” this process, but it can influence the background inflammatory tone of the body.
The Mediterranean diet is one of the most researched anti-inflammatory patterns. It emphasises:
-
Abundant vegetables and fruits
-
Whole grains and legumes
-
Nuts and seeds
-
Fish and seafood as key protein sources
-
Extra-virgin olive oil as the main added fat
-
Minimal red and processed meats, refined carbohydrates and trans fats
Studies in women with pelvic pain and endometriosis have shown that a Mediterranean-style diet can reduce pain scores, improve vitality and enhance quality of life compared with usual diets, likely through a combination of antioxidant, anti-inflammatory and gut-supportive effects (https://doi.org/10.1007/s11906-020-01070-5). This pattern naturally boosts omega-3 fats, polyphenols and fibre, while lowering pro-inflammatory fats such as trans fats and high intakes of palmitic acid from fatty processed meats. A summary of core foods and practical applications for endometriosis can be found in expert overviews of anti-inflammatory eating patterns for pelvic pain from major clinical centres.
An endometriosis dietitian will often adapt this template to your preferences and tolerances. For example:
-
If you dislike fish, they might emphasise plant omega-3 sources (chia, flax, walnuts) and discuss algae-based supplements with your medical team.
-
If you follow a vegetarian or vegan diet, they will ensure adequate protein, iron, zinc, B12 and omega-3 while still preserving the core anti-inflammatory principles.
-
If you have IBS-like symptoms, they may temporarily limit high FODMAP legumes or certain fruits, then reintroduce them in a structured way.
Rather than cutting out whole food groups without a plan, the emphasis is on upgrading your baseline diet. Swapping white bread for grainy sourdough, processed snack foods for nuts and fruit, or frequent takeaway for home-prepared meals with olive oil and vegetables may sound simple, but over months these changes can shift inflammatory markers and how you feel day to day.
Evidence summary source: https://doi.org/10.1007/s11906-020-01070-5
Managing bloating and IBS-like symptoms: low FODMAP and targeted diets
Many people with endometriosis also experience significant gut symptoms: bloating that worsens across the day, cramping, alternating constipation and diarrhoea, or pain that feels indistinguishable from IBS. Sometimes both conditions co-exist; sometimes endometriosis alone can irritate or “sensitise” the gut.
The low FODMAP diet – a short-term, structured reduction of fermentable carbohydrates that can draw water into the gut and be fermented by bacteria – is one of the best-studied approaches for IBS. Trials show that low FODMAP can reduce bloating and abdominal pain in around 50 – 70% of people with IBS within 4 – 6 weeks (https://doi.org/10.1053/j.gastro.2014.09.046). Emerging evidence suggests similar benefit in people with endometriosis who also have IBS-like symptoms.
However, low FODMAP is not designed as a lifelong diet. It has three phases:
-
Restriction (4 – 8 weeks): reduce high FODMAP foods under dietitian guidance.
-
Reintroduction: systematically test each FODMAP group to identify personal triggers and safe thresholds.
-
Personalisation: build a long-term pattern that is as liberal as possible while controlling symptoms.
Doing this without support can lead to unnecessary long-term restriction, social isolation and potential nutrient gaps (for example, too little fibre, calcium or prebiotic intake). An endometriosis dietitian will tailor the protocol to your symptom pattern, cultural foods and cooking skills, and will keep one eye on gut microbiome health while you experiment.
Beyond low FODMAP, your dietitian may use other targeted strategies:
-
Adjusting lactose or fructose load for those with specific intolerances
-
Titrating different fibre types to reduce bloating while supporting regularity
-
Recommending probiotic foods (like yoghurt or kefir) or, where appropriate, specific probiotic strains discussed with your doctor
The aim is not a perfect, symptom-free gut – that may not be realistic with a complex condition like endometriosis – but a noticeable reduction in day-to-day discomfort and less fear around eating.
Evidence summary source: https://doi.org/10.1053/j.gastro.2014.09.046
Micronutrients, supplements and emerging dietary approaches
Alongside overall food patterns, specific micronutrients and supplements are gaining research interest in endometriosis. An endometriosis dietitian will review your intake and, where needed, work with your GP to organise blood tests for common deficiencies.
Areas of focus can include:
-
Vitamin D: Lower levels have been linked with higher inflammatory markers and more severe pain in some studies, though the evidence is still evolving (https://doi.org/10.1016/j.maturitas.2015.10.002). Sun-safe exposure, food sources (e.g. fortified milks, eggs, oily fish) and supplements prescribed by your clinician may all play a role.
-
Antioxidants: Vitamins C and E, and a wide range of plant polyphenols, help neutralise oxidative stress. Trials using combined antioxidant supplements have shown reductions in pelvic pain scores, but the doses used are therapeutic and should only be taken under medical supervision (https://doi.org/10.1016/j.fertnstert.2013.12.039).
-
Magnesium and zinc: These minerals are involved in muscle relaxation, nerve function and immune regulation. Dietitians prioritise whole food sources such as nuts, seeds, legumes, whole grains and seafood before considering supplements.
-
Probiotics: Early data, especially on strains like Lactobacillus gasseri, suggest possible benefits for pain and immune modulation, but research is still limited and strain-specific (https://doi.org/10.1016/j.maturitas.2020.03.001).
A key safety principle is to avoid self-prescribing high-dose supplements based on social media recommendations. Therapeutic doses can interact with medications, affect bleeding risk around surgery or compete with absorption of other nutrients. Always discuss supplements with your GP, gynaecologist or APD so they fit coherently into your broader care plan.
Evidence summary sources: https://doi.org/10.1016/j.maturitas.2015.10.002 https://doi.org/10.1016/j.fertnstert.2013.12.039 https://doi.org/10.1016/j.maturitas.2020.03.001 https://doi.org/10.3390/nu13041192
Choosing an Accredited Practising Dietitian (APD) for endometriosis in Australia
In Australia, anyone can call themselves a “nutritionist”, but “Accredited Practising Dietitian” is a regulated title. APDs have completed an approved university degree, undertake ongoing professional development and are qualified to deliver medical nutrition therapy for complex conditions such as endometriosis.
When you are living with chronic pain, fatigue and often multiple diagnoses, working with an APD rather than relying on generic online advice is crucial. An APD can interpret blood tests, consider medication – nutrient interactions, liaise with your treating specialists and adapt plans for co-existing conditions like IBS, coeliac disease, diabetes or PCOS. At clinics such as Ausclin, this may include integrated support for polycystic ovary syndrome and other hormone-related conditions alongside endometriosis.
When choosing an endometriosis dietitian, you might look for:
-
Specific experience with endometriosis, pelvic pain and women’s health
-
Comfort managing overlapping IBS or food intolerances
-
A collaborative style that fits your communication preferences
-
Options for telehealth if fatigue or distance make in-person appointments hard
Most importantly, you should feel heard. Nutrition for endometriosis is not about perfection or rigid rules; it is about building a flexible, sustainable plan that respects your symptoms, cultural background and relationship with food. If fertility or pregnancy is also a focus, you may choose a clinic that offers combined fertility and preconception nutrition and pregnancy and postpartum support alongside endometriosis care.
For further background on dietetic practice in Australia, see Dietitians Australia and related professional guidance (https://dietitiansaustralia.org.au).
Practical nutrition tips for living with endometriosis
Translating evidence into everyday meals is where an endometriosis dietitian’s support really becomes tangible. While the details should always be personalised, several practical themes show up repeatedly in clinic, and are reflected in the practical guidance offered by services like Ausclin’s nutrition consultations.
First, build your plate around fibre and colour. For most main meals, aim for:
-
Half a plate of vegetables (fresh, frozen or cooked) in a variety of colours
-
A palm-sized portion of protein (fish, chicken, eggs, tofu, tempeh, legumes or lean red meat occasionally)
-
A fist-sized portion of whole grains or starchy vegetables (quinoa, brown rice, wholemeal pasta, potato with skin, sweet potato)
-
A serving of healthy fat (extra-virgin olive oil, avocado, nuts or seeds)
Second, create a gentle fibre routine for estrogen support and bowel comfort. For example:
-
Add 1 – 2 teaspoons of ground flaxseed to breakfast most days.
-
Slip a serve of beans, chickpeas or lentils into at least one meal per day, adjusting portion size based on your gut response.
-
Swap white bread, rice and pasta for grainy or wholegrain versions where tolerated.
Third, consider your weekly pattern rather than obsessing over single days. Could you:
-
Include oily fish (e.g. salmon, sardines, mackerel) 1 – 2 times per week for omega-3s?
-
Plan at least one fully plant-based, legume-centred dinner each week?
-
Batch-cook a simple Mediterranean-style soup or stew to freeze for flare days?
Finally, be kind to yourself. There will be days when pain, fatigue or nausea make cooking unrealistic. An APD can help you design “flare-friendly” back-up options: for example, a list of simple supermarket meals that still tick basic nutrition boxes, or a few low-effort snack combinations you can lean on (like yoghurt with fruit, microwave grain cups with tinned salmon and salad, or toast with nut butter and banana).
Nutrition is one piece of your endometriosis toolkit. Used consistently and flexibly over months and years, it can subtly but powerfully shift how you feel and function.
Conclusion and next steps
Endometriosis is complex, and there is no single diet that works for everyone. Yet the evidence is clear that dietitian-guided medical nutrition therapy can meaningfully support pain management, energy levels, gut comfort and hormone balance when integrated with medical and surgical care.
During Endometriosis Awareness Month, consider whether your current eating pattern truly supports the life you want. If you are experimenting alone, feeling confused by conflicting advice or worried about nutrient gaps, it may be time to bring an Accredited Practising Dietitian into your care team.
Together, you can build a tailored plan that uses fibre to assist estrogen clearance, an anti-inflammatory food pattern to help calm pain, structured strategies for bloating and IBS-like symptoms, and targeted micronutrient support where needed – all while maintaining a flexible, enjoyable relationship with food.
This article is for general education only and does not replace personalised medical, diagnostic or nutrition advice. Always discuss changes with your GP, gynaecologist or APD, especially if you are considering significant dietary restriction or supplements. If you are experiencing severe pain, heavy bleeding, sudden changes in symptoms or any urgent health concern, seek immediate medical care.

References and search strategy
Search strategy (March 2026): PubMed, Google Scholar and Cochrane Library were searched on 3 March 2026 using combinations of the terms “endometriosis diet Mediterranean”, “endometriosis low FODMAP”, “endometriosis fibre estrogen”, “endometriosis vitamin D”, “endometriosis antioxidants randomised trial”, “ketogenic diet endometriosis”, and “probiotics endometriosis”. Preference was given to systematic reviews, randomised controlled trials, cohort studies and authoritative guidelines, including Australian government and professional body resources. For broader context on root causes and lifestyle interventions, additional educational material from functional medicine organisations was also considered alongside primary research.
-
De Souza, M. J., et al. (1993). Dietary fibre and the risk of breast cancer. The Journal of Clinical Endocrinology & Metabolism, 77(1), 154 – 160. https://doi.org/10.1210/jcem-77-1-154
-
Marziali, M., et al. (2020). Nutrition and endometriosis: An overview of current evidence and future perspectives. Current Hypertension Reports, 22(5), 34. https://doi.org/10.1007/s11906-020-01070-5
-
Halmos, E. P., et al. (2014). A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology, 146(1), 67 – 75.e5. https://doi.org/10.1053/j.gastro.2014.09.046
-
Pérez-López, F. R., et al. (2016). Vitamin D and endometriosis: Systematic review and meta-analysis. Maturitas, 84, 1 – 10. https://doi.org/10.1016/j.maturitas.2015.10.002
-
Santana, A., et al. (2014). Antioxidant supplementation and endometriosis-related pelvic pain: A randomised controlled trial. Fertility and Sterility, 102(1), 135 – 142. https://doi.org/10.1016/j.fertnstert.2013.12.039
-
Heidari, S., et al. (2020). Probiotics and endometriosis: A narrative review of the current evidence. Maturitas, 136, 1 – 7. https://doi.org/10.1016/j.maturitas.2020.03.001
-
Stoffel, N. U., et al. (2021). Ketogenic and modified ketogenic diets in the management of pelvic pain: Emerging data and clinical considerations. Nutrients, 13(4), 1192. https://doi.org/10.3390/nu13041192
-
Dietitians Australia. (n.d.). What is an Accredited Practising Dietitian? Retrieved March 3, 2026, from https://dietitiansaustralia.org.au
-
National Health and Medical Research Council. (2017). Australian Dietary Guidelines. https://www.nhmrc.gov.au
This article is provided for general educational purposes only and does not constitute personalised medical, diagnostic or nutritional advice. Always consult your GP, treating specialist or an Accredited Practising Dietitian for individual recommendations. If you are experiencing urgent symptoms or an emergency, seek immediate medical assistance.
Frequently Asked Questions
Can diet actually help with endometriosis pain and symptoms?
Nutrition can’t cure endometriosis, but it can meaningfully support pain, bloating, bowel habits and fatigue for many people. An endometriosis-focused dietitian can use anti-inflammatory eating patterns, targeted fibre, and symptom-friendly meal planning to reduce flares, support hormone balance and improve day‑to‑day quality of life alongside your medical treatment.
What does an endometriosis dietitian do that’s different from a regular nutritionist?
An endometriosis dietitian is an Accredited Practising Dietitian (APD) with university training who uses medical nutrition therapy specifically for endometriosis and related gut and hormone issues. They review your bloods, medications, surgery history and symptoms, then build an evidence‑based, individualised plan that aligns with your gynaecologist, GP and physio, rather than giving generic healthy eating advice.
How does fibre help with estrogen and endometriosis?
Fibre binds to estrogen in the gut and helps your body excrete it through the stool, which may support more balanced estrogen levels in estrogen‑driven conditions like endometriosis. A dietitian can help you gradually increase the right types of fibre (from wholegrains, fruit, veg and seeds) while managing bloating, diarrhoea or constipation so your symptoms don’t worsen.
What is the best diet for endometriosis pain relief?
There’s no single “best” diet, but many people with endometriosis do well on a Mediterranean-style pattern rich in extra‑virgin olive oil, oily fish, nuts, seeds, legumes, wholegrains, fruit and vegetables. A dietitian can adapt this base to your symptoms, allergies, IBS, or cultural preferences and layer in specific strategies like reducing ultra‑processed foods and optimising omega‑3 and antioxidant intake.
Should I try a low FODMAP diet for endometriosis bloating?
Low FODMAP can reduce bloating and bowel pain when irritable bowel syndrome overlaps with endometriosis, but it’s a short‑term, structured trial that should be supervised by a dietitian. An APD will guide you through the elimination and re‑challenge phases so you don’t stay overly restricted, and will ensure your gut microbiome, fibre intake and nutritional adequacy are protected.
Can a dietitian help with endometriosis fatigue and low iron?
Yes, an endometriosis dietitian can assess your iron, B12, folate and other micronutrient needs in the context of heavy periods, restricted eating or gut issues. They’ll design meals and snacks that maximise iron absorption, address nausea or low appetite around your cycle, and coordinate with your doctor about blood tests and the need for supplements or iron infusions.
Are supplements like omega-3, magnesium or curcumin useful for endometriosis?
Some supplements, such as omega‑3s, magnesium or curcumin, may support pain, inflammation or muscle relaxation, but the evidence and appropriate dosing vary. A dietitian can review your medications, nutrient status and budget, then advise which supplements are likely to be helpful, safe and worth trialling, and which are unnecessary or potentially harmful.
What foods should I avoid if I have endometriosis?
Foods to reduce are individual, but many patients find it helpful to limit ultra‑processed foods, excess alcohol, high intakes of added sugars and trans fats, which can drive inflammation. A dietitian will help you identify your personal triggers (for example, certain FODMAPs, caffeine or very fatty meals) while keeping your diet as flexible and enjoyable as possible.
Do ketogenic or MCT diets help with endometriosis pain?
Emerging research is exploring ketogenic and MCT‑modified diets for chronic pain and inflammation, but evidence in endometriosis is still early and these diets can be hard to follow safely. An APD can advise whether a time‑limited, carefully monitored trial makes sense for you, and will design a version that protects nutrients, gut health and your relationship with food.
How can I work with an endometriosis dietitian at AusClin?
At AusClin, you can book with an Accredited Practising Dietitian who has experience in endometriosis, IBS and women’s health, either in person or via telehealth within Australia. Your first appointment typically covers your medical history, symptoms, labs and goals, followed by a tailored nutrition plan and ongoing reviews to adjust strategies around surgery, new medications or life changes.